

Why Emotional Intelligence Is Healthcare AI’s Hardest Problem
Lessons from a GITEX Panel on Clinical Technology

“Please do not tell my mother she has cancer.”
Professor Mehdi Soufi hears this request constantly in his practice in Morocco. Patients arrive with their elderly parents. The diagnosis is clear. The family makes a plea: do not burden them with this knowledge. Let them live in peace.
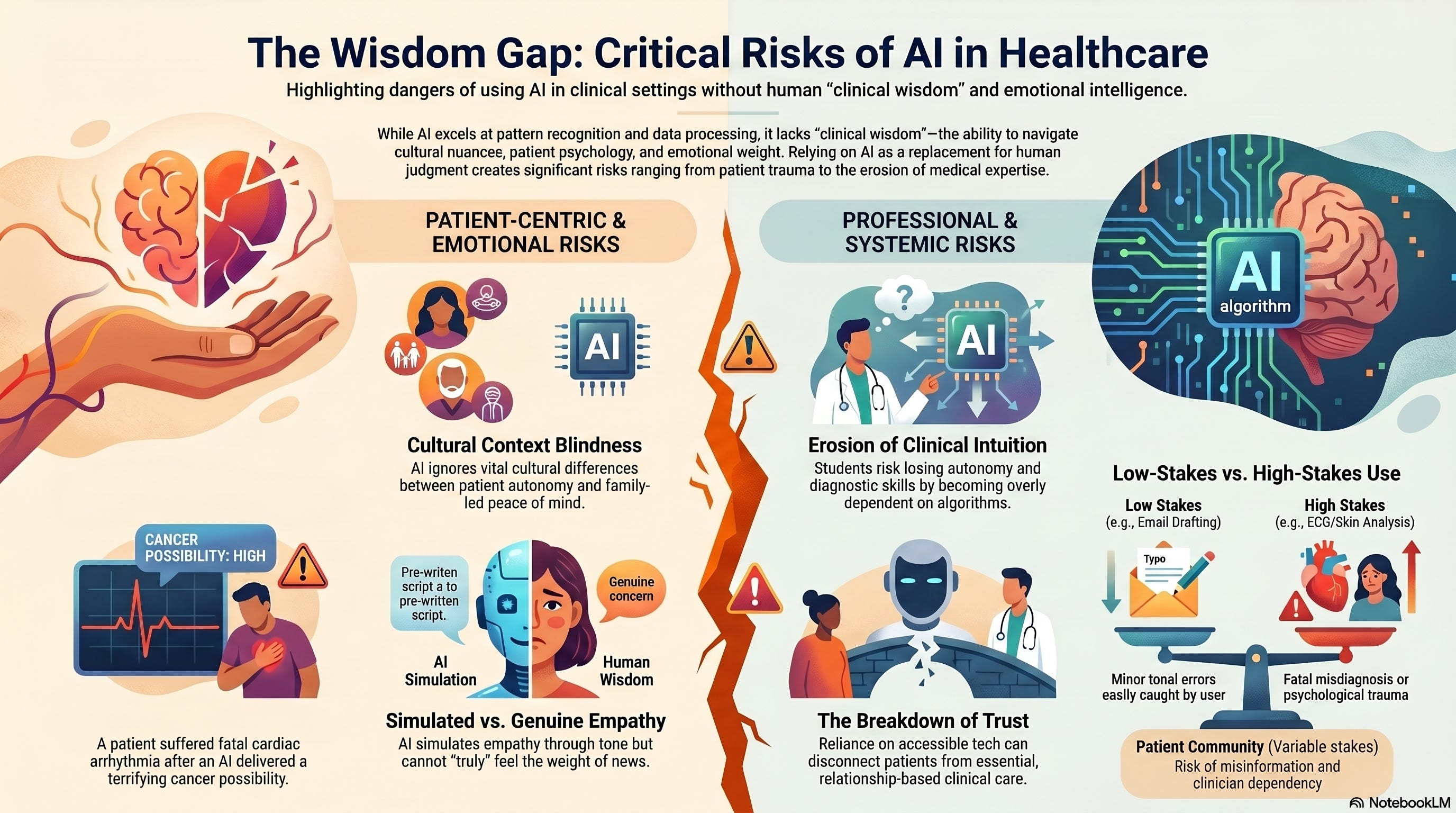
In France, Soufi explained, the culture is different. The patient has a right to know. The patient must know how to fight the disease, understand treatment, and make informed decisions. Full disclosure is not just standard practice; it is considered essential to patient autonomy.
Both approaches are rooted in care. Both aim to protect the patient. They are just protecting different things: in one case, the right to information; in the other, the right to peace of mind.
Now imagine an AI system delivering that diagnosis. Same algorithm. Same confidence level. Same recommendation. But radically different outcomes depend on cultural context, family dynamics, patient psychology, and dozens of other factors that the algorithm cannot see.
This is why emotional intelligence might be the hardest unsolved problem for healthcare AI.
The Diagnosis That Killed
At the panel I moderated a few weeks ago in Casablanca, Professor Soufi shared a case that haunts the promise of AI-driven healthcare: a patient in France entered his symptoms into an AI diagnostic tool. The system flagged cancer as a possibility. The patient panicked. His heart raced. He developed a fatal cardiac arrhythmia.
He did not have cancer.
The AI was not technically wrong. Given the symptoms, cancer was a reasonable differential diagnosis worth investigating. But the system had no way to calibrate how to communicate that risk. It could not assess whether this particular patient would spiral into panic. It could not sense that this person needed reassurance alongside information, that the delivery mattered as much as the data.
“AI does not judge people,” Soufi said. “It treats everyone the same way. It can announce a diagnosis to everyone in the same way. We need to be very careful because some people, when they hear something, are terrified.”
This is not an edge case. This is the fundamental challenge: healthcare is not just about accurate diagnosis. It is about delivering that diagnosis in a way the patient can metabolize.
The Simulation That Is Not Real
During the panel discussion, an audience member asked about using AI to assist with diagnosis while keeping physicians in control of treatment decisions. It was a reasonable compromise: let AI help with pattern recognition, but preserve human judgment for what matters most.
That is when I intervened with a distinction that needs to be made explicit: “AI can simulate emotional intelligence, but it does not feel emotion. And that is the difference.”
Rabia Cozijn, who survived cancer and now builds patient community platforms, reinforced this from the patient side. “I am a human being; I am very emotional,” she said. “I need to know that there is someone who is not just going to be giving me facts but truly understands how I am feeling when they are treating me.”
The word “truly” does the work there. AI can be programmed to sound empathetic. It can recognize emotional cues in text or voice. It can adjust its tone. But it cannot feel what the patient is feeling. It cannot experience the weight of delivering bad news or the relief of sharing good news.
And patients know the difference.
What Gets Lost When Students Stop Thinking
Professor Soufi’s concern extends beyond patient care to medical education. As dean of the medical faculty in Agadir, he watches students grow dependent on AI in ways that worry him.
“Students now, when you ask a question, they are already in listening mode to respond,” he said. “They are anticipating. There is a loss of autonomy. The day the internet stops, we will all be stuck.”
He was not romanticizing the past or resisting useful technology. He uses AI himself for email drafts, for presentation slides, and for literature reviews. But he distinguishes between AI as a tool and AI as a crutch.
When a student watches an AI diagnose a dermatological condition from a photo and generate a prescription, what is that student learning? They are learning to trust the algorithm. They are not learning to examine skin lesions, ask about family history, consider differential diagnoses, or develop clinical intuition.
“I try to show them real clinical cases,” Soufi explained. “Because each person is unique, each person has a story. You have to be with the person, accompany them through their entire healing trajectory, and be there for them. And I do not think a computer will ever do that.”
The Six Forms of Trust
When I asked Rabia Cozijn what keeps her up at night building health technology for African patients, she did not talk about technical challenges. She talked about trust and the six ways it can break:
She worries about reliability: patients becoming dependent on systems that might not be available when needed.
She worries about algorithms: patients over-relying on predictions without understanding their limitations.
She worries about misinformation: patients believing falsehoods because they align with their worldview rather than questioning scientific truth.
She worries that the platform could become the trusted partner in contexts where doctor-patient ratios reach 1:2000 or 1:3000, far beyond the 1:300 ratios in Western countries.
She worries about community risk: the spread of misinformation about health through patient networks that rely on shared experience rather than clinical guidance.
And she worries about dependency: patients disconnecting from clinicians because technology feels more accessible.
Each of these risks exists because healthcare is fundamentally a relationship among patient and provider, individual and community, and hope and reality. AI can process information. It cannot navigate relationships.
The Invisible Success Metric
Amine Moussaoui, who manages Morocco’s blood transfusion systems, offered perhaps the most sophisticated success metric I have heard in healthcare IT: “The day clinicians stop talking about the information system is the day we have succeeded.”
He was not advocating for systems so automated that humans become unnecessary. He was describing systems so well-designed that they integrate seamlessly into clinical workflow, augmenting judgment without demanding attention.
But achieving that requires what Moussaoui called “alignment of three dimensions”: technology capabilities, business processes, and user workflow. Miss anyone, and the system fails, not because it is technically inadequate, but because it does not fit how care actually gets delivered.
“A system is only used if users trust it,” Moussaoui said. “We are talking about trust in the data, but also trust in availability, trust that the system is robust and proven.”
That trust is not earned through accuracy metrics or uptime statistics. It is earned through systems that demonstrably help clinicians work “better, more calmly, and more accurately,” Moussaoui’s framing of what healthcare IT should actually deliver.
The Question AI Cannot Answer
Near the end of the panel, Professor Soufi posed a question to the audience: “Who will trust a prescription from a computer that only reads an ECG? Who will trust a dermatology diagnosis from scanning a skin lesion into an algorithm?”
Some hands went up. Not many.
Then he asked: “Who uses AI to write emails?”
Nearly every hand in the room shot up.
The difference is not technical capability. AI can read ECGs and analyze skin lesions with high accuracy. The difference is consequence and context.
Email is low-stakes. If the AI gets the tone slightly wrong, you edit it. If it misses nuance, you catch it. The cost of error is minimal.
Healthcare is high-stakes. If the AI misreads a cardiac rhythm or misclassifies a lesion, someone could die. And unlike email, you often lack the expertise to know when the AI is wrong.
But even more than the consequences, the difference lies in the relationship. An email comes from you. A diagnosis comes from a system and is delivered to someone in a vulnerable moment, someone who needs not just information but reassurance, not just accuracy but care.
The Partnership, Not the Replacement
In her closing statement, Rabia Cozijn captured what the entire conversation had been circling: “It has to be a partnership. It cannot be exclusivity.”
AI and human intelligence are working together, not one replacing the other. Algorithms augment clinical judgment, not substitute for it. Technology provides tools, not takes over the relationship between healer and patient.
Dr. Ouattara reinforced this from the systems side: “Data alone will not be enough for decision-making. We need to put the user at the center. The decision must be at the center of what we do.”
And Professor Soufi brought it back to the fundamental truth: “Each person is unique. Each person has a story. You have to be with them, accompany them. A computer will never do that.”
This is not Luddism. Everyone on that panel uses AI. Everyone sees its value. But they also see what it cannot do and what gets lost when we pretend otherwise.
What We Are Actually Asking
The question is not whether AI will transform healthcare. It already has.
The question is whether we can deploy it in ways that preserve what makes healthcare human: the ability to read not just data but emotion, to calibrate not just accuracy but delivery, to build not just efficiency but trust.
Because emotional intelligence is not a nice-to-have feature we can add later. It is the foundation of care itself. It is how clinicians know when to push and when to comfort, when to disclose and when to protect, when to act and when to wait.
AI can simulate those responses. It cannot generate them from genuine understanding.
And until we stop pretending that simulation is sufficient, we will keep building systems that optimize for everything except what patients actually need: someone who not only knows what is wrong but also cares about what happens next.
That is the difference between artificial intelligence and human wisdom. And it is why the humans in the loop are not just a safety feature; they are the point.
This concludes the three-part series on lessons from the “Clinical Tech: Force Multiplier for Care” panel at GITEX Future Health Morocco 2026.
Ousmane Diallo is the author of “The Cognitive Revolution.” His work explores how intelligent systems reshape decision-making in organizations and societies.