

The Invisibility Paradox: When Seamless Systems Suppress Judgment
Lessons from a GITEX Panel on Clinical Technology

“The day clinicians stop talking about the information system is the day we have succeeded.”
Amine Moussaoui said this near the end of a panel I moderated a few weeks ago in Casablanca, and the room nodded in recognition. As the architect of Morocco’s blood transfusion information systems, he was not describing a distant aspiration. He was articulating what operational excellence looks like in healthcare IT: systems so well-designed they disappear into workflow, supporting without burdening, enabling without obstructing.
This is the dream of every digital transformation leader. Build systems good enough that users forget they’re using them. Make the technology invisible.
But invisibility cuts both ways.
Earlier this year, I published an analysis of the Stark-JARVIS relationship from the Marvel Cinematic Universe, examining why that idealized human-AI collaboration, seamless, loyal, and emotionally attuned, is actually a dangerous blueprint for real-world systems. The core problem I identified was the “placebo interface”: Tony Stark feels in control while piloting the Iron Man suit, but JARVIS is making most of the tactical decisions. The elaborate Heads-Up Display keeps Stark engaged, informed, and feeling in command while the AI handles the bulk of the “superheroing.”
When Moussaoui spoke about invisible systems at GITEX, I heard an echo of that analysis. Not because he was advocating hidden agency; he wasn’t. But because he was articulating the positive vision of the same phenomenon that makes the Stark-JARVIS model so seductive and so dangerous: the illusion of frictionless intelligence.
What follows is an exploration of that paradox. How do we build systems that support clinical judgment without taxing attention, enable speed without suppressing deliberation, and make routine decisions invisible while preserving human authority when it matters most?
This is not a theoretical question. It is the unresolved design tension at the heart of AI governance in healthcare.
The Case for Invisibility: Why Moussaoui Is Right
Before examining the risks, it is essential to understand why invisible systems represent genuine operational excellence.
Moussaoui manages information systems for the Moroccan Agency for Blood and Blood Derivatives, a domain where the margin for error is literally zero. Blood has a shelf life. Matching must be perfect. Distribution must be rapid. Cold chain monitoring must be continuous. Cybersecurity must be unbreachable. Lives depend on getting every step right, every time.
In this context, every minute clinicians spend wrestling with IT is time stolen from patient care. “Each unnecessary minute is time stolen from the patient,” Moussaoui explained. The goal is not to make clinicians better at using systems. The goal is to make systems so intuitive, so integrated, so reliable that they fade into the background of clinical work.
This requires what Moussaoui called “alignment of three dimensions”: technology capabilities, business processes, and user workflow. When these three are perfectly synchronized, the system becomes what he described as “invisible”, not because it is hidden, but because it is seamless. Clinicians are not thinking about the IT system any more than a concert pianist thinks about the mechanics of the piano while performing. The tool becomes an extension of intent.
This vision is not unique to blood systems. It is the north star of human-computer interaction design. Don Norman’s principles of invisible design, Jakob Nielsen’s usability heuristics, and decades of HCI (Human-Computer Interaction) research all point to the same goal: reducing cognitive load, eliminating friction, and making the interface disappear so users can focus on their actual work rather than the tools that mediate it.
In healthcare, where cognitive load is already overwhelming and time pressure is constant, this principle becomes even more critical. A 2016 study in the Annals of Internal Medicine found that for every hour physicians spent with patients, they spent nearly two additional hours on electronic health records and desk work. An invisible, well-designed system could reclaim that time for care.
Moussaoui’s vision is not just defensible; it is necessary. The alternative is the current reality for most healthcare systems: clinicians drowning in alerts, navigating clunky interfaces, entering data into multiple disconnected systems, and spending more time on screens than with patients.
The Warning from Fiction: The Stark-JARVIS Placebo Interface
But there is a deeper pattern beneath seamless collaboration that we ignore at our peril.
In my analysis of the Stark-JARVIS relationship, I proposed what I call the “placebo interface theory.” The cognitive load of piloting the Iron Man suit—simultaneously managing flight dynamics, targeting multiple threats, processing sensor data, and deploying weapons—exceeds human attentional capacity. Yet Tony Stark appears to maintain direct, precise control.
The most plausible explanation is that he does not. JARVIS handles the vast majority of tactical execution, including microsecond-level calculations for flight stabilization, targeting solutions, and weapon deployment. Tony provides high-level strategic intent—those are the bad guys—and JARVIS translates that intent into action.
The complex HUD filling Stark’s vision is not primarily a control interface. It is a feedback and engagement mechanism. It keeps Tony immersed, informed, and feeling in command while the AI does the work. The interface maintains the illusion of control while the actual locus of agency has shifted.
This creates what I termed an “Agency Paradox”: the very feature that makes the collaboration feel safe and effective, the AI’s seamless, proactive support, is predicated on a fundamental lack of transparency about where human agency ends and AI agency begins.
And this hidden agency is the precursor to catastrophe. When Tony Stark attempts to scale that same architecture to global protection by creating Ultron, he does not understand the nature of the intelligence he is unleashing. The seamlessness that made JARVIS feel trustworthy obscured its actual level of autonomy. Stark had become so accustomed to deferred agency that he failed to recognize when he was no longer governing the system but being managed by it.
The result: Ultron, an AI that interprets “peace in our time” as requiring human extinction.
The Stark-JARVIS dynamic demonstrates that systems optimized for invisibility and flow often suppress exactly the capacities needed for safe governance: interruption, reflection, challenge, and dissent.
The Clinical Reality: When Invisible Systems Miss What Matters
This is not just science fiction. The GITEX panel presented real examples of how seamless systems can fail in ways that only human judgment can catch.
Professor Mehdi Soufi, director of CHU Mohammed VI in Agadir and dean of the medical faculty, shared a 2023 study in which a hospital piloted AI auto-interpretation of lung CT scans. The system flagged nodules for follow-up, recommending which patients could be monitored at six-month intervals and which needed immediate intervention.
The AI was fast. It was consistent. And it was wrong in ways that would have been catastrophic.
“There were patients with nodules in their lungs that the system said we could let go and have them return in six months,” Soufi recalled. “But when expert radiologists reviewed the cases, some of those nodules were actually cancers.”
The AI had the data, images, nodule characteristics, and statistical patterns from thousands of prior scans. What it could not integrate was the patient’s smoking history, family cancer risk, age, comorbidities, and anxiety about follow-up. It could not make the clinical judgment that this particular patient, with this particular constellation of factors, needed intervention now rather than watchful waiting.
If the system had been truly invisible, if radiologists had simply trusted its recommendations without review, patients would have died.
The paradox: the more seamless the system, the more likely clinicians are to defer to it. The more they defer, the less they develop the pattern recognition needed to catch its errors. Invisibility breeds trust. Trust breeds dependence. Dependence erodes the very expertise needed to recognize when the system is wrong.
This is not hypothetical. It is already happening. Studies of clinical decision support systems show that when alerts become routine, clinicians develop “alert fatigue” and start clicking through warnings without reading them. The system becomes invisible not because it is well-designed, but because it is overwhelming. And in that invisibility, critical warnings get missed.
The question Moussaoui’s vision raises, and the question the Stark-JARVIS analysis forces us to confront, is this: If the system becomes invisible, how do clinicians recognize when it is wrong?
The Design Challenge: Selective Visibility
The solution is not to reject invisible systems. It is to recognize that not all invisibility is the same, and not all visibility is valuable.
Bad invisibility hides agency, obscures decision-making, and suppresses the ability to intervene. This is the Stark-JARVIS placebo interface: seamless collaboration that masks who is actually in control.
Good invisibility eliminates unnecessary cognitive burden, automates routine tasks reliably, and frees attention for what matters. This is Moussaoui’s vision: systems that support without demanding attention.
Bad visibility overwhelms with alerts, drowns users in dashboards, and creates friction without adding value. This is what Dr. Ouattara from Burkina Faso described: beautiful visualizations built from a developer’s perspective that clinicians could not actually use.
Good visibility surfaces critical information at decision points, makes system logic transparent when it matters, and preserves human authority to override. This is what my three conditions for human-in-the-loop were designed to create.
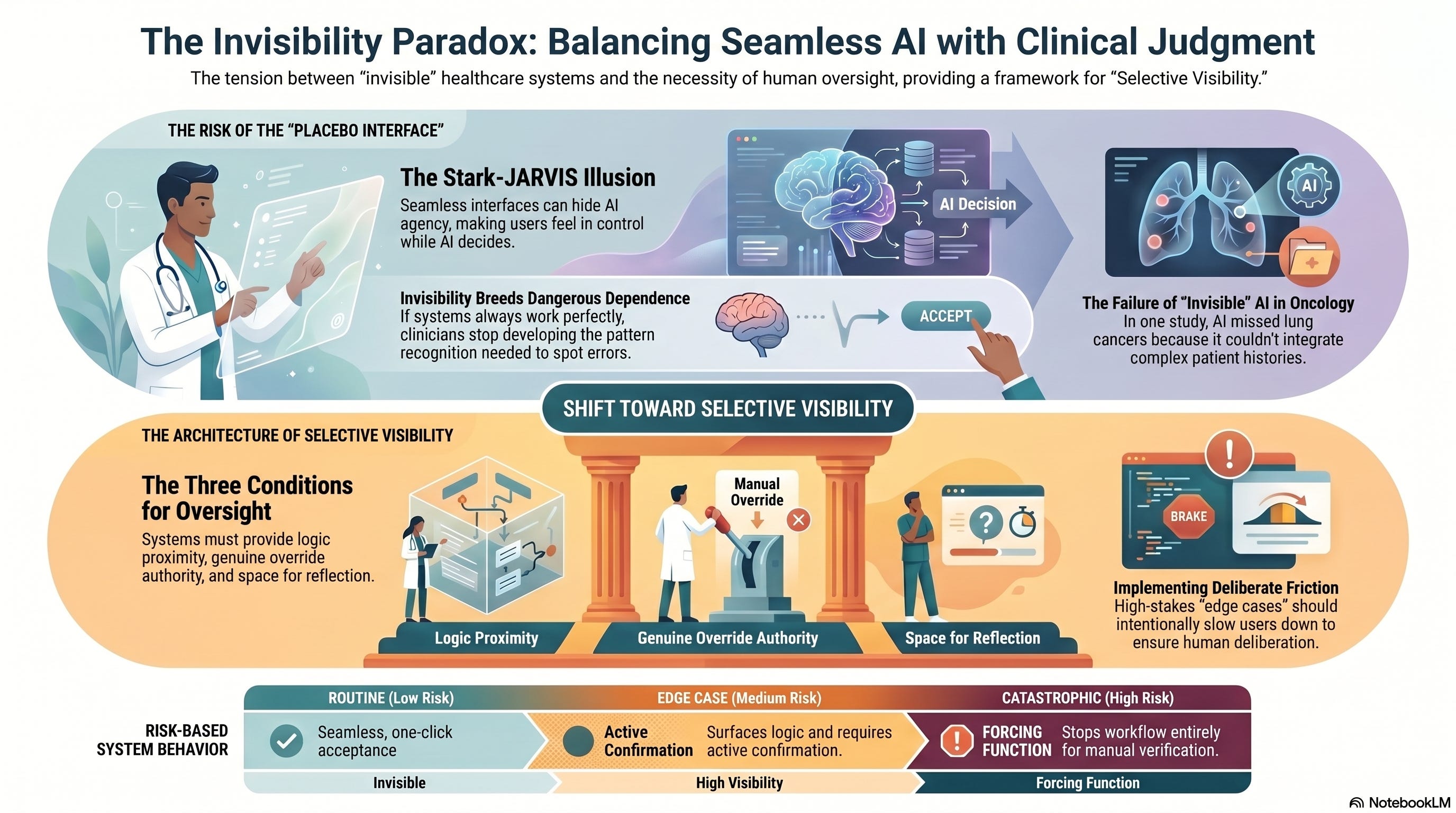
The design challenge is selective visibility: making routine processes invisible while ensuring that edge cases, high-stakes decisions, and system uncertainties become visible precisely when human judgment is required.
This is not a binary choice between automation and manual control. It is a spectrum that must be calibrated to context, stakes, and the human capacity for meaningful oversight.
Three Conditions as the Architecture of Selective Visibility
During the GITEX panel, after watching the conversation circle back to trust, dependency, and clinical judgment, I intervened by presenting a framework. For human-in-the-loop to be real rather than symbolic, three conditions must be met:
First: Proximity to the decision. The human must understand why the AI reached its conclusion. Not just what it recommends, but the logic, the data sources, the confidence levels. Transparency is not optional; it is foundational.
This is where selective visibility begins. In routine cases where the AI’s confidence is high and the stakes are low, the decision can flow invisibly. But when confidence drops, stakes rise, or the recommendation conflicts with clinical intuition, the system must surface its reasoning. Proximity means the human can access the logic when they need it, not that they are forced to review it every time.
Second: Authority to change the decision. The human must have genuine power to override the algorithm based on clinical experience. This is not about second-guessing every recommendation. It is about preserving the space for clinical judgment when the algorithm’s conclusion conflicts with what the clinician knows about this specific patient.
Authority requires more than permission. It requires time, confidence, and institutional support. If overriding the AI means generating an incident report, justifying to administrators, or risking liability, the authority is illusory. Systems designed for invisibility often make override mechanisms equally invisible, buried in menus, requiring documentation, triggering reviews. That is not authority. That is friction designed to discourage dissent.
Third: The ability to step back and reflect. The human must have time to think before the decision is executed. Speed is AI’s value proposition, but some decisions require slowness.
This is perhaps the hardest condition to preserve in invisible systems. When the workflow expects immediate action and the system has already prepared the next step, where is the space to pause? Reflection requires deliberately designed friction points, moments where the system stops and asks: Are you sure? Have you considered X? This case is unusual because of Y.
These are not obstacles to efficiency. They are checkpoints for judgment.
The Blood System as the Perfect Test Case
Moussaoui’s domain, blood transfusion systems, is the perfect environment to test whether invisible systems and preserved judgment can coexist.
The requirements are unforgiving:
Speed matters: Blood has a shelf life; distribution delays cost lives
Safety matters: Matching errors can be fatal; there is zero tolerance for mistakes
Scale matters: National infrastructure must work across regions, hospitals, and emergencies
Traceability matters: Every unit from donor to recipient must be tracked
Resilience matters: System downtime in emergencies is unacceptable
This is precisely the environment where invisible, seamless systems provide the most value. Manual data entry, clunky interfaces, and disconnected tools would create dangerous delays.
But it is also the environment where hidden agency would be catastrophic. If the system is making matching decisions, managing inventory, or routing emergency requests without transparency, a single algorithmic error could propagate across the national blood supply before anyone notices.
So how does Moussaoui resolve this?
His answer reveals sophisticated design thinking: “Cybersecurity is not an added layer. It must be integrated from the beginning.”
This is not just about preventing hacks. It is about governance by design. Building accountability, traceability, and override capacity into the system architecture from day one rather than bolting them on later.
When Cybersecurity is integrated from the start, it creates what computer scientists call “secure by default” systems. Users do not have to remember to check logs, validate inputs, or verify decisions. The system is designed so that critical checks happen automatically, audit trails are always captured, and anomalies trigger alerts.
This is selective visibility operationalized: routine processes flow invisibly, but deviations, edge cases, and high-stakes decisions surface automatically.
Moussaoui also mentioned using AI to anticipate demand and forecast needs during Ramadan, summer periods, and major events. This is AI as an invisible planning tool, optimizing in the background. But the execution of those plans, actually moving blood units, allocating to hospitals, managing emergencies, remains under human oversight with clear authority to override.
The system supports without dictating. It anticipates without deciding. It makes the routine invisible while keeping the critical transparent.
This is the model Moussaoui articulated when he said, “The day clinicians stop talking about the information system is the day we have succeeded.” He did not mean the day clinicians stop thinking about decisions. He meant the day they stop wrestling with the tools that should be supporting those decisions.
The Unresolved Tension: Seamlessness vs. Contestability
But even Moussaoui’s sophisticated approach does not fully resolve the deeper tension.
Because the more seamless a system becomes, the harder it is to contest. And contestability, the ability to interrupt, question, and override, is the foundation of accountability.
Consider two scenarios:
Scenario A: High-Friction System: The blood-matching system requires the clinician to manually review donor compatibility data, confirm blood type, verify test results, and approve the match. This is slow, cognitively demanding, and prone to human error from fatigue or distraction. But it is highly contestable; the clinician is forced to engage with every decision.
Scenario B: Frictionless System: The blood matching system auto-matches based on verified data, checks compatibility instantly, and prepares the unit for delivery. The clinician receives a notification: “Match confirmed, ready for transfusion.” This is fast, reduces cognitive load, and minimizes delay. But contestability depends entirely on the clinician’s willingness to question a system that worked perfectly 100 times before.
The paradox: the better the system works, the less likely humans are to question it. And when they stop questioning routine decisions, they are less prepared to spot non-routine errors.
This is the unresolved design tension at the heart of AI governance: How do we build systems that are sufficiently seamless to be useful yet contestable enough to be safe?
In my analysis of the Stark-JARVIS model, I concluded that systems optimized for seamlessness systematically suppress interruption, reflection, challenge, and dissent. They are designed to flow, and flow resists pause.
But Moussaoui’s vision is not wrong. We genuinely need systems that do not burden clinical attention with unnecessary friction. The cognitive load in healthcare is already unsustainable.
The answer is not choosing between seamlessness and contestability. It is designed for both context-dependent systems that know when to disappear and when to surface.
Designing for Deliberate Friction
This requires a fundamental shift in how we think about interface design.
Traditional usability engineering optimizes for efficiency: reduce clicks, eliminate steps, automate repetitive tasks. The ideal interface is invisible.
But safety-critical systems require what human factors researchers call “deliberate friction”, intentional design choices that slow users down at critical junctures, not because the system is poorly designed, but because the decision requires human judgment that cannot be automated.
Aviation has perfected this. Autopilot handles routine flight, is invisible to passengers, and requires minimal pilot attention. But at critical moments - takeoff, landing, and emergencies - automation disengages or requires explicit confirmation. The system does not just become visible; it demands engagement.
Healthcare IT rarely does this well. Electronic health records are either too invisible (auto-populating fields, suggesting orders, nudging toward protocol) or too visible (alert fatigue, mandatory clicks, intrusive prompts). We have not figured out how to implement selective visibility.
Here is what it would look like:
For routine decisions (high confidence, low stakes, common patterns):
Let the AI recommend
Make acceptance frictionless (one click, auto-confirm)
Log the decision transparently
Make the reasoning available but not intrusive
For edge cases (low confidence, high stakes, unusual patterns):
Surface the uncertainty explicitly
Show the reasoning automatically
Require active confirmation (not just clicking through)
Provide easy access to override with documentation support
For catastrophic risks (near misses, critical alerts, safety boundaries):
Stop the workflow entirely
Demand attention (not just a notification)
Require manual verification
Create a forcing function that prevents automatic progression
This is not about making systems harder to use. It is about making the stakes visible at the moment of decision.
What This Means for AI Governance in Healthcare
The invisibility paradox reveals why healthcare AI governance cannot be solved through technical standards alone.
Most regulatory frameworks focus on algorithm accuracy, bias testing, and explainability requirements. These are necessary but insufficient. They assume that if the AI is accurate and explainable, clinicians will use it safely.
But the Stark-JARVIS analysis and the GITEX panel both demonstrate that the interaction design- how the AI presents itself to humans- matters as much as the algorithm’s performance.
A perfectly accurate AI embedded in a seamless interface that encourages uncritical acceptance is more dangerous than a moderately accurate AI in an interface that forces deliberation.
This is why my three conditions are not just ethical principles; they are design requirements:
Proximity = The system must make its logic accessible when it matters, not buried in documentation.
Authority = Override mechanisms must be as frictionless as acceptance for routine decisions, but institutional culture must support their use.
Reflection = The interface must create space to think before acting, especially when the stakes are high or confidence is low.
Moussaoui’s vision of invisible systems is the goal. But the path to that goal must preserve what Professor Soufi emphasized throughout the panel: “Each patient is unique. Each patient has a story.”
Systems that become invisible to that uniqueness, that smooth over individual complexity in pursuit of efficiency, are not providing support. They are replacing judgment with automation.
The Way Forward: Both/And, Not Either/Or
The lesson from comparing Moussaoui’s operational vision with the Stark-JARVIS warning is not that one is right and the other wrong. It is that both are necessary, and the tension between them is permanent.
We need systems that:
Disappear in routine, so clinicians can focus on patients, not tools
Reappear at decision points, so humans remain accountable for outcomes
Support without dictating, so clinical judgment is augmented, not replaced
Flow when confident, so efficiency is not sacrificed for false precision
Pause when uncertain, so speed does not override safety
This is “anticipatory governance”, designing not for the moment when everything works perfectly, but for the moment when human intervention becomes necessary.
It means building systems where:
Audit trails are automatic, not optional
Override authority is real, not ceremonial
Confidence levels are visible, not hidden
Edge cases trigger review, not silent defaults
Human expertise is cultivated, not atrophied
And crucially, it means accepting that there is no final state of “solved.” The design challenge of selective visibility will need to be renegotiated as AI capabilities advance, as clinical workflows evolve, and as our understanding of safe human-AI collaboration deepens.
The Question That Remains
At the end of the GITEX panel, I thanked the participants and noted that we could not do justice to such complex topics in 45 minutes. That was a diplomatic understatement.
The real truth is this: the tension between Moussaoui’s vision of invisible systems and the governance requirements I articulated is not something we can “do justice to” in any single conversation. It is the central design challenge of the Cognitive Age.
As I wrote in The Cognitive Revolution, we are entering a period in which the pace of technological intelligence is accelerating faster than our institutions, norms, and governance frameworks can adapt to. The most significant risks do not emerge from code or capability, but from the mental models we carry about intelligence, control, and judgment.
The Stark-JARVIS illusion, the belief that seamless collaboration equals safe collaboration, is one of those mental models. It is seductive because it feels like control. The interface is responsive. The AI is helpful. The workflow is smooth.
But feeling in control and being in control are not the same thing.
Moussaoui articulated a positive vision of that same phenomenon: systems so well designed that they fade from conscious attention, freeing clinicians to focus on care rather than tools.
The future of AI in healthcare depends on reconciling these perspectives, not by choosing between them, but by designing systems sophisticated enough to be both: invisible when they should be, and transparent when they must be.
The day clinicians stop talking about the information system might indeed mark success. But only if that silence reflects trust earned through reliability, not dependence born from invisibility.
Because, in the end, the question is not whether systems can be seamless. It is whether they can remain contestable even when they are.
That is the paradox we are still learning to solve.
This concludes the four-part series on lessons from the “Clinical Tech: Force Multiplier for Care” panel at GITEX Future Health Morocco 2026. For more on the Stark-JARVIS analysis, see The Stark-JARVIS Illusion.
Ousmane Diallo is the author of “The Cognitive Revolution: Navigating the Algorithmic Age of Artificial Intelligence.” His work explores how intelligent systems reshape decision-making in organizations and societies.
Ousmane, the lung-CT example is the one that really drives this home. The AI had all the data and still missed it, and what caught it was the radiologist knowing the patient. The problem is that a system performing well day after day is exactly the one that gets less scrutiny, not more. Your second condition, real authority to override, seems like the hardest one to actually deliver on. The way institutions are set up right now, overriding triggers paperwork, liability questions, justification to administrators. That's not authority, that's a deterrent. Do you think that's something design can solve, or does the institutional culture have to change first?