

The Diagnostic Vacuum: How Scarcity Transforms Care

Healthcare failures rarely begin with bad decisions.
They begin with a missing capacity.
When people imagine diagnostic error, they often picture a mistake: a misread scan, a missed symptom, a flawed judgment.
But in modern healthcare systems, especially outside the Global North, many failures occur before judgment is even possible.
They occur in what can be called the diagnostic vacuum: the widening space between human need and clinical attention.
Diagnosis Requires Presence
Diagnosis is not a single act.
It is a process that depends on:
Time,
Continuity,
Contextual knowledge,
And human presence across moments.
Historically, diagnosis emerged through repeated encounters, clinicians noticing change over time, recognizing deviation from baseline, and holding uncertainty long enough for clarity to emerge.
That model is eroding globally.
In high-income countries, it erodes under overload.
In low- and middle-income countries, it erodes under absence.
Scarcity Is Structural in the Global South
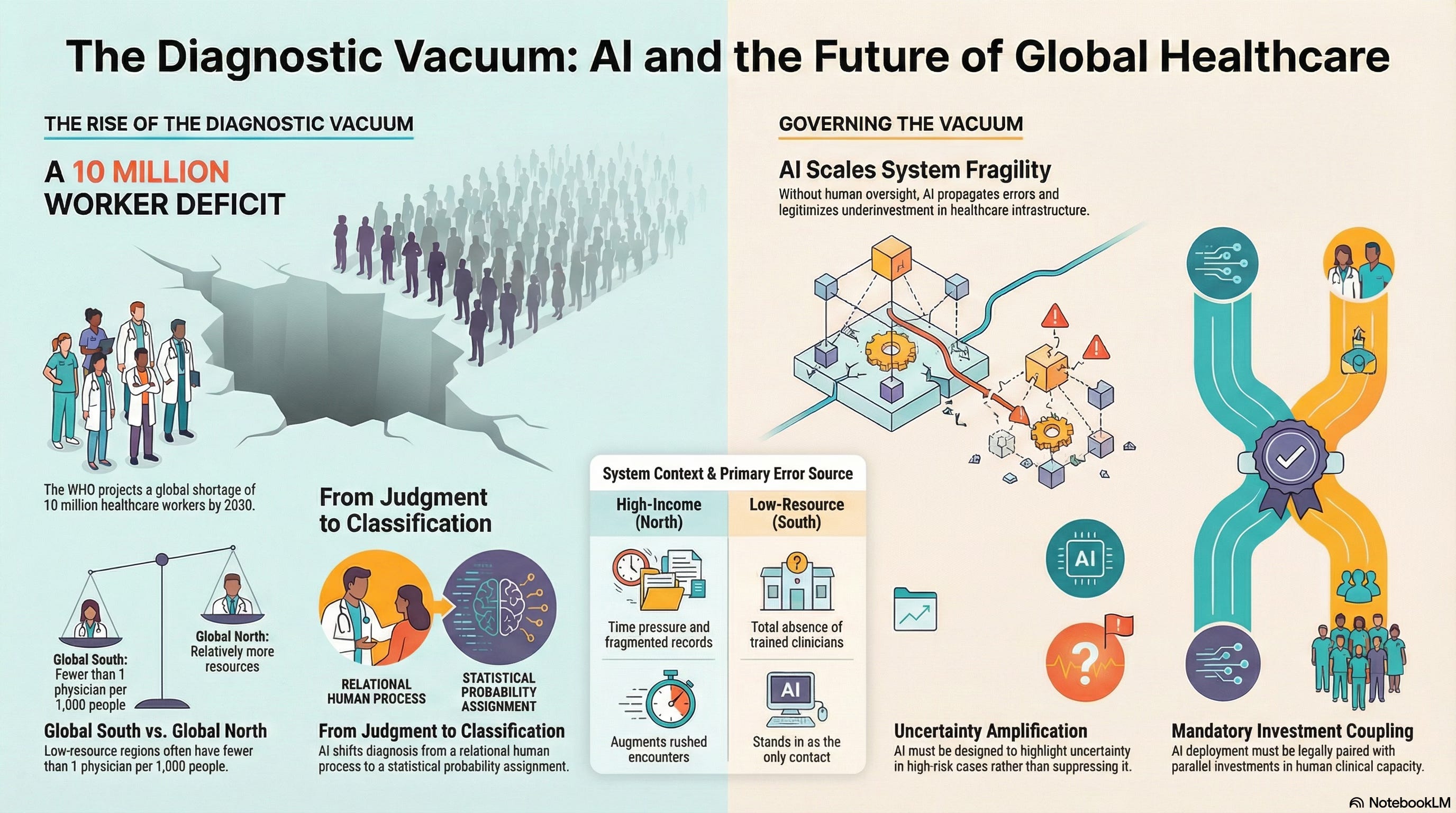
According to the World Health Organization, the world faces a projected shortage of 10 million healthcare workers by 2030, with the vast majority of that deficit concentrated in the Global South.
In many countries:
Physician density falls below 1 per 1,000 people, compared to 2.5–4 per 1,000 in much of the Global North
Entire regions lack specialist care altogether
Diagnostic imaging, pathology, and longitudinal records are unavailable or inaccessible
Globally, nearly half the world’s population lacks access to essential health services.
In these contexts, diagnosis is not delayed.
It is missing.
The diagnostic vacuum is not a gap between appointments.
It is a structural condition.
The Future is a choice.
This work is open to everyone. Free subscribers have full access to all writing and research.
Paid and founding subscriptions exist solely to support the work itself, helping preserve independent thinking focused on human judgment, governance, and responsibility in the Cognitive Age.
Scarcity Does Not Just Delay Care; It Rewrites It
When systems cannot meet demand, they adapt.
In the Global North, adaptation often looks like:
compressed visits,
algorithmic triage,
decision support layered onto rushed encounters.
In the Global South, adaptation looks different:
task-shifting to community health workers,
episodic care without records,
and increasing reliance on mobile or AI-mediated tools as the only point of contact.
In both cases, scarcity reshapes diagnosis.
But in low-resource settings, AI is not augmenting diagnosis; it is often standing in for it.
The Rise of AI as a First, and Sometimes Only, Diagnostician
Mobile symptom checkers, chatbot-based triage, and automated risk assessment tools are rapidly expanding in regions with a scarcity of clinicians.
These systems are often justified on humanitarian grounds:
Scale,
Reach,
And cost efficiency.
In many cases, they provide value.
But they also redefine what diagnosis becomes when:
No clinician is available,
No follow-up is guaranteed,
And no escalation path exists.
Diagnosis shifts from interpretation to classification.
From relational judgment to probability assignment.
The diagnostic vacuum is filled with inference rather than understanding.
Diagnostic Error Looks Different Under Absence
In high-income systems, diagnostic error often stems from:
Time pressure,
Fragmented records,
Premature closure.
In low-resource systems, diagnostic failure often stems from:
Lack of diagnostics entirely,
Absence of trained clinicians,
And the inability to revisit decisions.
AI does not correct these conditions.
It normalizes them.
A statistically “reasonable” output can mask the fact that no human system exists to catch errors, contextualize risk, or absorb moral responsibility.
AI Scales What Exists, Including Fragility
This is the core risk.
AI scales capacity, but it also scales the structure in which it is embedded.
In fragile systems, this means:
Errors propagate without correction,
Confidence replaces verification,
And harm surfaces late, if at all.
A diagnostic system that works “well enough” statistically can still be devastating in environments where:
Misclassification has no recourse.
And uncertainty cannot be revisited.
The vacuum hardens.
The Human Cost Is Uneven and Predictable
In the Global South, the diagnostic vacuum produces:
Delayed or absent diagnoses,
Preventable disease progression,
And deepening mistrust in formal health systems.
In the Global North, it produces:
Clinician burnout,
Defensive medicine,
And moral injury from practicing under impossible constraints.
In both cases, AI is introduced as a means of relief.
In both cases, without governance, it risks becoming a structural substitute.
Governance Must Be Context-Sensitive
Most AI governance frameworks are implicitly Global North–centric.
They assume:
Existing clinical infrastructure,
Available human oversight,
And functioning escalation pathways.
These assumptions do not hold globally.
Effective governance must ask different questions depending on context:
Where no clinician exists, what decisions must AI never make alone?
What uncertainty thresholds require referral, even if referral capacity is scarce?
How do we prevent AI from legitimizing underinvestment in human systems?
These are not technical questions.
They are political and ethical ones.
Designing Against Permanent Absence
There are concrete safeguards that matter, especially in low-resource settings:
Explicit scope limits on what AI may diagnose or recommend
Uncertainty amplification, not suppression, in high-risk cases
Mandatory referral triggers, even when capacity is limited
Investment coupling, where AI deployment requires parallel human capacity building
Auditability across contexts, not just model accuracy
Without these, AI risks becoming a technological justification for scarcity rather than a bridge beyond it.
A Cognitive Age Reckoning
The Cognitive Age is not just about intelligence.
It is about how intelligence is governed when human capacity is unevenly distributed.
The diagnostic vacuum reveals a hard truth:
AI does not merely respond to scarcity.
It renders scarcity legible and, at times, permanent.
If we fail to govern this dynamic, we will confuse reach with care, and classification with understanding.
That mistake will be felt first in the Global South.
And eventually, everywhere.