

From Data to Decisions: Why Healthcare AI Keeps Failing the “So What?” Test
Lessons from a GITEX Panel on Clinical Technology

Dr. Jean Serge Dimitri Ouattara has a problem that most health systems would envy: too much data.
As Director of Information Systems for Burkina Faso’s Ministry of Health, he oversees the deployment of many digital health tools across one of the world’s most resource-constrained health systems. These tools generate rivers of data, community health workers recording patient encounters, clinics logging visits, vaccination programs tracking coverage, and disease surveillance systems monitoring outbreaks.
The data exists. It flows into servers. It populates dashboards. And then… nothing.
“We created accounts for all our partners and told them: just go into DIS2, you have the data,” Ouattara explained at a panel I moderated a few weeks ago in Casablanca. “But with the multitude of data scattered across the system, it was not practical. That was our first lesson: beyond collecting data, we need to identify which data is actually relevant to which actors.”
This is the quiet crisis in healthcare AI: we are generating more data than ever while making decisions no better than before.
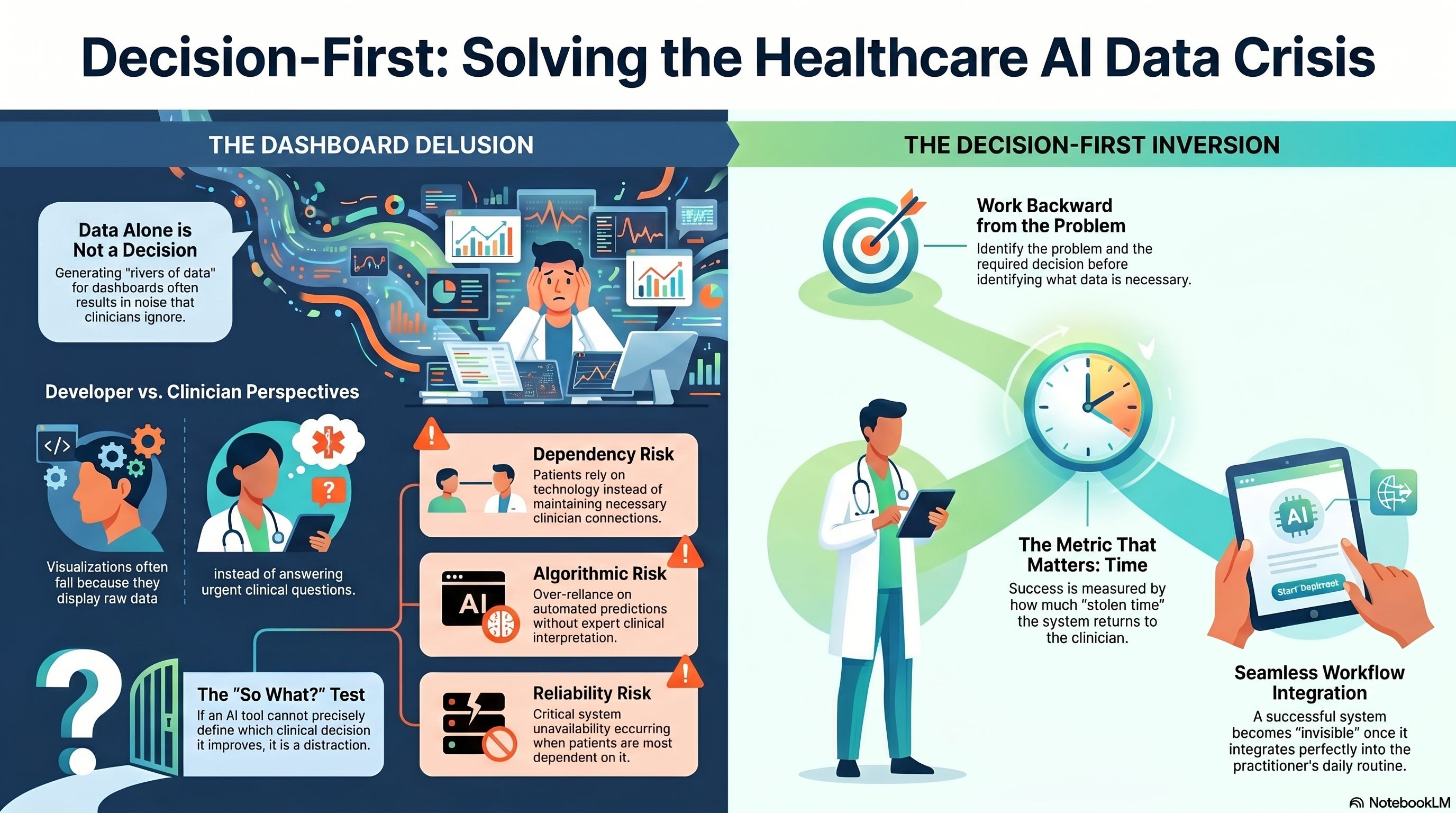
The Dashboard Delusion
Ouattara’s team tried to solve the problem the way most organizations do: they built dashboards. Beautiful ones. Charts, graphs, histograms, pie charts, everything a modern data visualization should include.
They scheduled meetings with stakeholders, proud to demonstrate their work on digitizing community health. “It was a complete failure,” Ouattara said plainly.
Why? Because the dashboards were built from a developer’s perspective rather than a clinician’s. The visualizations displayed data, but they did not answer clinical questions. Practitioners could not extract the information they needed to make decisions about patient care.
“Second lesson,” Ouattara continued, “we need to put the user at the center of modeling these dashboards.”
So they rebuilt. They worked with clinicians to identify which indicators mattered, how information should be presented, and how to make it accessible to practitioners with limited time and attention.
And they still were not done. Because even with user-centered dashboards showing relevant information, there was simply too much of it. Practitioners had information but still could not act decisively.
The Inversion
This is where Ouattara’s insight becomes critical for anyone deploying AI in healthcare.
“We realized we need to work backward,” he said. “We need to start with the decision instead of the data.”
Instead of asking “What data do we have?” they began asking: “What problem are we trying to solve? What decisions need to be made? What data is necessary to make those decisions? And how should that data be presented?”
The user defines the problem. The user defines the decision. Only then does the system identify which data matters and how to deliver it.
“We are moving from information systems to decision-support systems,” Ouattara explained. “Data alone is never enough for decision-making.”
This inversion, from data-first to decision-first, is the difference between AI systems that get ignored and ones that transform care.
When the Algorithm Cannot See the Patient
Professor Mehdi Soufi, director of CHU Mohammed VI in Agadir, gave this abstraction concrete form.
His hospital runs robotic surgery programs and has been piloting AI diagnostic tools since 2023. One study used AI to auto-interpret lung CT scans, flagging nodules for follow-up. The system made recommendations. Some were correct. Some were not.
“There were patients with nodules in their lungs that the system said we could let go and have them return in six months,” Soufi recalled. “But when expert radiologists reviewed the cases, some of those nodules were actually cancers.”
The AI had data, images, nodule characteristics, and statistical patterns from thousands of prior scans. What it did not have was the ability to integrate that patient’s smoking history, their family cancer risk, their age and comorbidities, and their anxiety level about follow-up. It could not make the clinical judgment that this particular patient, with this particular constellation of factors, needed intervention now rather than watchful waiting.
“It is a back-and-forth,” Soufi said. “We take what we can from the positives, but we have to filter out the negatives.”
But how do you “filter out the negatives” when the system is designed for efficiency, when the workflow expects speed, when the institution measures success by throughput?
The Six Risks No One Is Pricing In
Rabia Cozijn knows this tension from the patient side. After surviving cancer, she left her role leading digital transformation for South Africa’s national railway to build Anixi Health, a community platform for chronic illness patients across Africa.
When I asked her what keeps her up at night, building patient-centered technology in constrained contexts, she did not hesitate: dependency.
“What happens when the technology is interrupted or unavailable?” she asked. “We know 40-50% of patients in Africa struggle with medication adherence. So, we design systems to help them manage adherence. But what happens when that system goes down and they forget to take their medication? Are we assisting them or compounding the problem?”
She named six categories of risk that most AI deployment plans ignore:
Reliability risk: System unavailability when patients depend on it
Algorithmic risk: Over-reliance on predictions without clinical interpretation
Misinformation risk: Patients doing their own research, believing falsehoods that align with their worldview
Trust risk: In rural Africa, with 1:2000 patient-doctor ratios, the platform becomes the trusted partner
Community risk: False health information spreading through patient networks
Dependency risk: Patients relying on technology instead of maintaining a connection to clinicians
These are not edge cases. They are design constraints that should shape every decision about how AI gets embedded in care delivery.
“We need to make sure we are not just relying on algorithmic direction,” Cozijn emphasized. “We need to ensure clinicians are included in how information is interpreted and communicated to patients.”
The Metric That Actually Matters
Amine Moussaoui, who manages Morocco’s blood transfusion systems, offered the clearest measure of whether decision-support is working: “Every unnecessary minute is time stolen from the patient.”
In blood systems, this is literal. Blood has a shelf life. Matching must be perfect. Distribution must be rapid. Lives depend on speed.
But Moussaoui made a crucial distinction: the goal is not to optimize system metrics such as uptime, processing speed, or data completeness. The goal is to optimize clinical time and patient safety.
“The real question today is not whether the system works,” Moussaoui said. “It is what actually helps the clinician work better, more calmly, and more accurately.”
This requires aligning three dimensions: technology capabilities, business processes, and user workflow. “If these three are not aligned,” he noted, “no system will function for the patient’s benefit.”
When they are aligned, the system becomes invisible. “The day clinicians stop talking about the information system is the day we have succeeded,” Moussaoui said. Not because the system disappeared, but because it integrated so seamlessly into the workflow that it no longer demands attention.
The Question Before the Algorithm
Before deploying any AI system in healthcare, Ouattara’s inversion offers a forcing function: What decision is this helping make?
Not “what data will this generate,” or “what efficiency will this create,” or “what capability will this demonstrate.” What actual clinical decision will be different, and better, because this system exists?
If you cannot answer that question precisely, you are building a dashboard that will be ignored, an algorithm that will be worked around, or a dependency that will fail patients when it matters most.
The proliferation of healthcare data creates the illusion that we are approaching better decisions. But data without a decision focus is just noise with a bigger storage bill.
As Ouattara put it in his closing: “Data alone will not be enough for decision-making. We need to reverse the process. What problem do we want to solve? What decisions can be made? What data is necessary? What are the biases involved?”
Then, and only then, should we build the Algorithm.
Because the alternative is not just a wasted investment. It is clinicians drowning in dashboards they do not trust, patients depending on systems that might not be there when needed, and decisions being made faster without being made better.
That is not clinical technology as a force multiplier. That is clinical technology as a distraction from what actually improves care.
Next in this series: What happens when cultural differences, not just technical ones, determine whether AI recommendations get followed. And why emotional intelligence might be healthcare AI’s hardest unsolved problem.
Ousmane Diallo is the author of “The Cognitive Revolution” and moderated the “Clinical Tech: Force Multiplier for Care” panel at GITEX Future Health Morocco 2026.