

Beyond the Buzzword: What “Human-in-the-Loop” Actually Requires
Lessons from a GITEX Panel on Clinical Technology

“Human-in-the-loop” has become the default answer whenever someone questions AI autonomy in healthcare. The phrase appears in ethics guidelines, procurement requirements, and conference presentations. It reassures us that humans remain in control even as algorithms accelerate clinical decisions.
But at a panel I moderated last week at GITEX Future Health in Casablanca, a simple question exposed how shallow that reassurance often is: What does it actually take for human-in-the-loop to be real rather than symbolic?
When Theory Meets Practice
The panel brought together four practitioners running health systems across Africa: Professor Mehdi Soufi, director of Morocco’s most technologically advanced teaching hospital; Dr. Jean Serge Dimitri Ouattara, leading digital health strategy in Burkina Faso; Rabia Cozijn, building a patient community platform after surviving cancer herself; and Amine Moussaoui, managing Morocco’s blood transfusion systems, where errors have zero tolerance.
Each operates in contexts where AI promises genuine relief from workforce shortages, administrative burden, and infrastructure fragmentation. These aren’t academic debates about future possibilities. These are live decisions about systems already mediating care.
Professor Soufi opened with a surgeon’s bluntness: “Will anyone go to a hospital to be treated by a robot and say, ‘go ahead, treat me’? Who will do that?” The room laughed, but the question was not rhetorical. Hospitals are already deploying AI for triage, diagnosis support, and treatment recommendations. The question is not whether AI will be embedded in clinical decisions; it already is. The question is what role humans actually play once the algorithm has spoken.
The Panic That Killed
The conversation took a darker turn when Professor Soufi shared a case from France: a patient entered his symptoms into an AI diagnostic tool. The system flagged cancer. The patient panicked, developed tachycardia, and died. He didn’t have cancer.
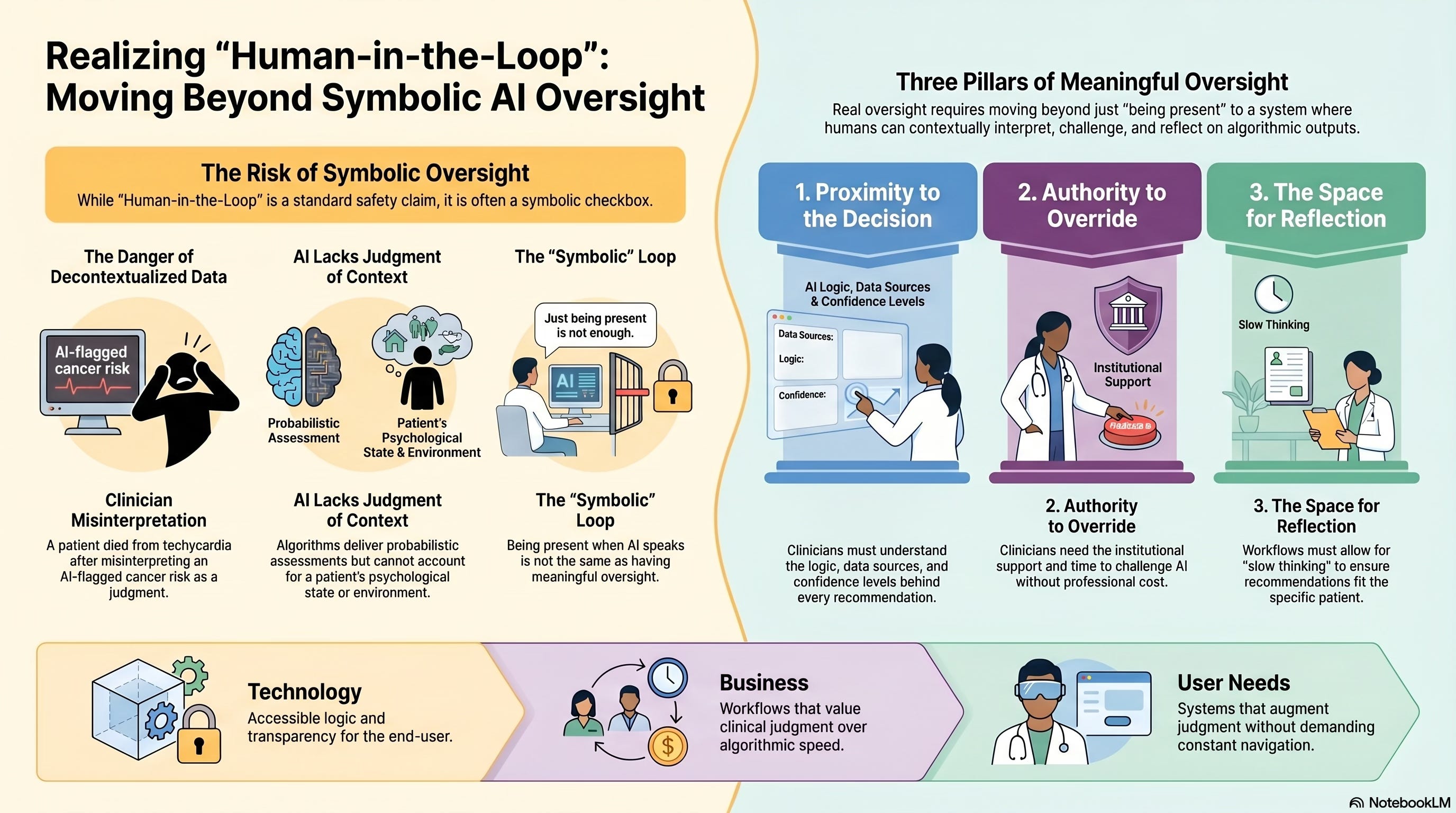
The AI wasn’t technically wrong to flag the possibility based on symptoms. But it had no way to account for the patient’s psychological state, his family context, his ability to process frightening information. It delivered a probabilistic assessment as if it were a definitive judgment. The patient treated it as such.
“AI does not judge context,” Soufi said. “It treats everyone the same way. It can announce a diagnosis to everyone in the same way. But we need to be very careful because some people, when they hear something, are terrified.”
This is where the standard “human-in-the-loop” defense collapses. Yes, a human was technically “in the loop”, the patient himself. But he had no training to interpret algorithmic output, no clinical experience to contextualize risk, no relationship with the system to build trust in its limitations.
Being present when AI speaks is not the same as having meaningful oversight.
Three Conditions for Real Oversight
After watching the conversation circle around trust, dependency, and clinical judgment for thirty minutes, I intervened with a framework:
For human-in-the-loop to be real rather than symbolic, three conditions must be met:
First: Proximity to the decision. The human must understand why the AI reached its conclusion. Not just what it recommends, but the logic, the data sources, the confidence levels. Transparency is not optional; it is foundational. If the clinician cannot explain why the algorithm suggested this path, they cannot meaningfully endorse or override it.
Dr. Ouattara from Burkina Faso had lived this failure. His ministry deployed dashboards displaying data from many fragmented digital health tools. The dashboards were beautiful, with charts, graphs, and real-time updates. Clinicians ignored them. Why? Because they were built from a developer’s perspective rather than a clinical one. “The dashboards did not allow clinicians to extract the clinical information they needed,” he explained. “We had to completely rebuild them, putting the user at the center.”
Proximity means the system’s logic must be accessible to the person who will be held accountable for the outcome.
Second: Authority to change the decision. The human must have genuine power to override the algorithm based on clinical experience, not just theoretical permission. This is not about second-guessing every recommendation; that would paralyze workflow. It is about preserving the space for clinical judgment when the algorithm’s conclusion conflicts with what the clinician knows about this specific patient.
But authority requires more than permission. It requires time, confidence, and institutional support. If overriding the AI means generating an incident report, justifying to administrators, or risking liability, the “authority” is illusory. Clinicians will defer to the algorithm not because they trust it, but because challenging it is professionally costly.
Third: The ability to step back and reflect. The human must have time to think before the decision is executed. This is perhaps the hardest condition to preserve as systems accelerate. Speed is AI’s value proposition: faster triage, faster diagnosis, faster treatment decisions. But some decisions require slowness.
Rabia Cozijn, who survived cancer and now builds digital health platforms, named this tension directly. She worries that patients may become dependent on systems they cannot verify. “What happens when the technology is interrupted or unavailable? Are we assisting patients or compounding the problem?”
The same applies to clinicians. When the system suggests a path and the workflow expects immediate action, where is the space for the clinician to pause and consider whether this recommendation fits this patient?
The Invisible Success
Amine Moussaoui offered the most sophisticated measure of success I have heard: “The day clinicians stop talking about the information system is the day we have succeeded.”
He was not advocating for invisibility through automation. He meant that when systems are well-designed, they disappear into workflow. They augment judgment without demanding attention. They provide the right information at the right moment without requiring the clinician to navigate complexity or second-guess recommendations.
But achieving that invisibility requires relentless focus on alignment between technology capabilities, business processes, and user needs. “If these three dimensions are not aligned,” Moussaoui said, “no system will function for the patient’s benefit.”
The Question We Are Not Asking
Human-in-the-loop has become a checkbox, a way to signal that we have addressed the autonomy concern without wrestling with what meaningful oversight requires.
The three conditions—proximity, authority, and reflection—demand more than technical design. They demand an organizational culture that values clinical judgment over algorithmic efficiency. They demand workflows that create space for thinking, not just executing. They demand accountability structures that support override decisions rather than punish them.
Most importantly, they demand that we stop treating “human-in-the-loop” as the answer and start asking: Which humans? In which loop? With what power? At what cost?
Because the alternative is not just theoretical. It is the patient who panicked at an algorithm’s suggestion and died from fear of a cancer he did not have.
That is the cost of symbolic oversight disguised as meaningful control.
Next in this series: How Africa’s health systems are navigating AI deployment in contexts of extreme fragmentation and what they are learning about building decision-support that clinicians actually trust.
Ousmane Diallo is the author of “The Cognitive Revolution” and moderated the “Clinical Tech: Force Multiplier for Care” panel at GITEX Future Health Morocco 2026.
Not enough to just "be in the loop", I agree one Gotta be at the right place to make a meaningful impact.